
Thursday, February 28, 2013
Wednesday, February 27, 2013
Balantidium coli
Balantidium coli
The ciliate protozoa form a large group of organisms that is characterised by numerous cilia. A large number of ciliates are free-living and an equally large number consists of parasites of the digestive systems of termites, cockroaches and herbivores.
A typical ciliate has a conical mouth, the cytostome, near the anterior end and an anal opening, the cytopyge, at the posterior end. Ciliates have two types of nuclei: a large kidney-shaped macronucleus and a small spherical micronucleus, both of which are visible in the cyst and in the trophozoite.

Balantidium coli is the only ciliate that is parasitic to humans. Balantidium coli has a global distribution in pigs, dogs and several species of monkeys. In man, it occurs mainly in warm climates. The parasite occurs in the large intestine of man, pigs and monkeys.
Morphology
The parasite exists as a cyst and as a trophozoite, the trophozoite being the active form. It is ovoid and covered by cilia that are perpetually in motion, which are used for movement. The parasite varies in size, ranging from 50 to 100 µm in length by 40 to 70 µm in width. The anterior end is conical and the posterior end is rounded. To one side of the anterior end, there is funnel-like peristome, which leads to the cytostome or mouth.



Balantidium coli trophozoite (left) and cyst (right)
Life cycle
Balantidium coli lives in the large intestine where it feeds on bacteria, cells and food particles present in the intestinal lumen. Asexual reproduction is by binary fission in which the micronucleus first divides followed by the division of the macronucleus, resulting in two daughter organisms. B. coli can also reproduce sexually by a process called conjugation, which involves the exchange of nuclear material.

Life cycle of B. coli. A, ingestion of cyst; B, trophozoite formed in the colon divides by binary fission;
C, trophozoite in the lumen of the large intestine or in faeces freshly voided.
Pathogenesis
The effect of the infection in the pig is minimal, as the parasite does not seem to penetrate the mucosal surface. In humans and monkeys, the parasite can enter the surface of the large intestine causing extensive tissue erosion. Furthermore, the parasite may penetrate through the muscularis mucosae into the submucosa and spread out radially causing rapid destruction of the tissues. Most of the lesions caused by Balantidium coli are found in the caecal and sigmoid rectal regions.
The symptoms vary from severe diarrhoea and dysentery to mild insignificant, almost asymptomatic condition.
Epidemiology


Infection is acquired by the ingestion of cysts of Balantidium in food or water contaminated with faecal matter. Since balantidiasis is common in dogs and primates, it may be expected that these animals are probably the main source of infection to man. However, human infections are usually associated with people who come in contact with pigs, chiefly pig keepers or butchers.
The infection rate is very low in humans and this is because humans are generally refractory to exposure to Balantidium. However, once the infection has established itself in man, there is usually a rapid transmission from one person to another, particularly where there is no proper sanitation.
Diagnosis and treatment
Slide smears of infected faeces should show characteristic cysts or trophozoites of Balantidium coli. The infection responds to treatment with tetracycline, and metronidazole.
Leishmaniasis
Leishmaniasis
These haemoflagellates of the genus Leishmania are parasites of invertebrates and vertebrates that use small biting sand flies (Phlebotomus), such as P. sargenti, P. papatasii, P. argentipes and many others, depending on the geographical area as vectors. The leishmanias are rounded or oval parasites with a morphologically complex life cycle consisting of a promastigote with a free flagellum and amastigote that has no flagellum.
Human leishmaniasis is scattered over wide areas of the globe, from China Asia to India Iran Afghanistan Near East , the Mediterranean basin, into Sudan Ethiopia West Africa . In the New World , it extends fromMexico Argentina
The diseases attributed to Leishmania range from a mildly inconvenient lesion of the skin, known as Oriental sore, to a serious disease involving the liver and spleen, known as kala-azar. In South America , one form of leishmaniasis (mucocutaneous) extensively involves the mucous membranes of the mouth, nose and pharynx, as well as the skin but does not affect the viscera.
Leishmaniasis is a zoonotic disease that is maintained in nature by many animals including dogs, rodents, wolves, foxes, jackals, raccoons, sloths and marsupials. Numerous species of Leishmania have been described in mammals and of these three are generally accepted as human parasites; two of these cause cutaneous leishmaniasis and the third causes visceral leishmaniasis or kala-azar.
Life cycle, symptomatology and epidemiology
The amastigote forms of Leishmania are ingested by sand flies when they feed on the blood and tissue fluid of vertebrates. Compared with trypanosomes, development of Leishmania in the sand fly seems quite simple, involving the transformation of the amastigote forms to promastigotes. These promastigotes multiply in the digestive canal of the insect and transform into infective promastigotes which are injected into a new vertebrate host when the fly feeds again.

Life cycle
In the vertebrate the promastigotes enter host macrophage cells, roundup and lose their flagella, forming the so-called Leishman bodies or amastigote forms that are the characteristic forms found in the vertebrate. The parasites multiply and increase within the host cells until they cause them to rupture. The rapture of the host cells liberates more parasites that are engulfed by other phagocytic cells.
Table. Leishmania species and main characteristics associated with infections
Species
|
Characteristics
|
Major foci
|
L. aethiopica
|
Cutaneous, self-healing, also diffuse, zoonotic
| |
L. donovani
|
Visceral, kala-azar, anthroponotic
| |
L. infantum
|
Visceral, zoonotic (dogs)
| |
L. major
|
Cutaneous, self-limiting, rural, zoonotic
|
Mediterranean basin and
|
L. tropica
|
Cutaneous, self-healing, with possible recurring satellite lesions, urban, anthroponotic
|
Mediterranean basin and
|
L. braziliensiscomplex
|
Cutaneous and mucocutaneous, zoonotic
| |
L. chagasi
|
Visceral, zoonotic (dogs)
| |
L. mexicanacomplex
|
Cutaneous, and a few mucocutaneous reported in
| |
Cutaneous leishmaniasis (Oriental Sore)
Cutaneous Leishmaniasis is characterised by sores on the face, arms and legs especially in children. The aetiological agent isLeishmania tropica, a parasite that has a wide distribution in Asia , Middle East and Africa .
The classical lesion of cutaneous leishmaniasis is the Oriental Sore, which is about 5 to 15 cm in diameter and takes several months to develop following infection. Incubation period is usually between 2 to 7 months or longer. The infection is usually accompanied by spontaneous healing of the sore after 9 to 12 months, sometimes leaving unsightly scars on the skin. There is increasing evidence that the infection is followed by permanent immunity.
The sores do not usually contain pus except when they have been invaded by bacteria. Classical sores are found from the Mediterranean region to India Asia and parts of Africa . Another form of Oriental sore is the relatively wet one that attacks the lymph nodes. This has a shorter incubation period than the dry Oriental sore. It is probably a zoonosis since it occurs in rural areas where its reservoirs are dogs, ground squirrels and gerbils.
Mucocutaneous leishmaniasis (Espundia)
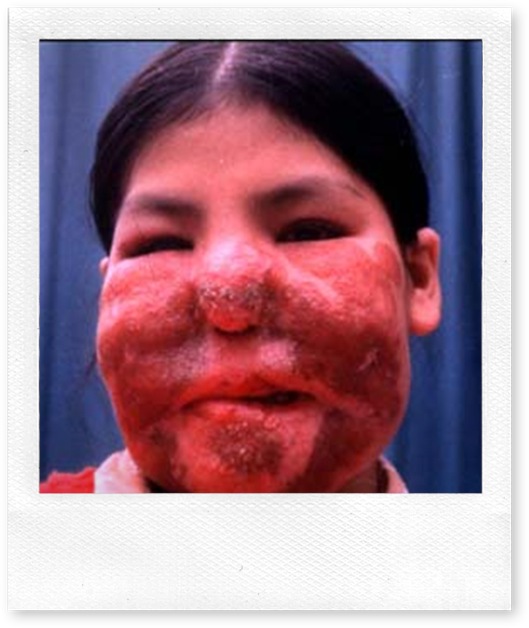
Mucocutaneous leishmaniasis is a chronic disease that occurs in Central and South America . The aetiological agent isLeishmania braziliensis and the most severe form of the disease is called espundia which is endemic in the jungles of South America , particularly Peru Bolivia Brazil

Oriental sore (A and B) and espundia (C)
Visceral Leishmaniasis (kala-azar)
Visceral leishmaniasis is caused by L. donovani, a parasite similar to both L. tropica and L. braziliensis. Visceral leishmaniasis exists in China India Afghanistan Sudan Ethiopia East Africa , South and Central America . It attacks the reticuloendothelial cells of the spleen, liver, bone marrow and visceral lymphatic nodes. This is a rural disease with dogs, foxes, rodents and other mammals acting as its reservoirs.
Biting sandflies introduce promastigotes into the dermal region of the skin. The promastigotes enter the blood and lymph vessels and make their way to the liver, spleen, and bone marrow via lymph and blood. As the parasites divide and increase in numbers, they cause the rupture of the macrophages and release of more parasites that become available to infect more macrophages. The destruction of the macrophages continues until their numbers are considerably reduced.
To counteract the loss of macrophages, the bone marrow is activated to produce more macrophages at the expense of other important cells such as polymorphonuclear cells. The resulting monocytosis and leucopoenia weaken the defence system of the body very badly. The result is that many of the victims of kala-azar succumb to infections that they would normally resist.
Clinical kala-azar develops when the liver, spleen, kidney, and bone marrow are infected. Very often kala-azar is fatal if not treated. In other people, however, the symptoms may assume a chronic course.
The symptoms of kala-azar include headaches, irregular bouts of fever with a temperature (which can range from 36 oC to 40 oC) and oedema of the face, trunk and feet. Other symptoms include substantial weight loss, splenomegaly, hepatomegaly, and anaemia, bleeding from the gums, lips, nose and intestinal mucosa.
Leishmania donovani exhibits geographical host-relationships. In China India
In the Mediterranean region where dogs are important reservoirs, children are usually more affected than the adults. In theSudan Sudan Americas Sudan Nile grass rat), Acomys albigena (the spiny mouse), the genet and the serval. In the semi - arid northern districts of Kenya Uganda
Diagnosis
In cutaneous leishmaniasis, the presence of parasites can be demonstrated in blood smears made from skin scrapings, aspiration of juice from the wound or biopsy. Alternatively, the scrapings from the lesion can be cultured or inoculated into hamsters and examined for the presence of amastigotes. In kala-azar, a biopsy from the bone marrow or spleen can be examined for the presence of amastigotes, cultured on a suitable media or inoculated into hamsters before being examined. In either case, the presence of amastigotes confirms the infection.
Treatment
Proper parasitological identification of the parasites is essential for correct treatment. This is because the treatment of leishmaniasis is long and the drugs are toxic. Cutaneous leishmaniasis is usually self-limiting and most of the wounds heal within 6-9 months. The infection can therefore be left to take its course until it heals, unless the wounds are disfiguring because of bacterial involvement. In many parts of southwest Asia , children are exposed to infection or given live virulent injections of the parasite in order to induce immunity that will protect them against further infection and thus avoid disfiguring lesions and scars on the face.


A case of kala-azar, with enlarged liver and spleen
Mucocutaneous leishmaniasis and kala-azar are more serious than cutaneous leishmaniasis because they are not only incapacitating they can also be fatal. The first line of treatment involves the administration of pentavalent antimonials, such as stibogluconate, or meglumine antimoniate. The second line drugs if the antimonials fail are amphoterin B and pentamidine. If untreated, kala-azar has a mortality rate of 100 %.
Vector Control
The diversity of the epidemiology of the different forms of the disease makes it impossible to control leishmaniasis with a single approach or tool. Infection can be prevented by use of repellents or insecticides against sandflies. The elimination of dogs and other reservoir hosts greatly reduces the risk of infection. Vector control using suitable insecticides are effective against peridomestic transmission.
Subscribe to:
Posts (Atom)